ascending cholangitis or acute cholangitis.

Bacterial infection of the biliary tree in the presence of complete or partial bile duct obstruction is called ascending cholangitis, acute cholangitis, bacterial cholangitis,
The CT findings that can be seen in patients with ascending cholangitis include
1-dilatation of the intra- and extrahepatic bile ducts,
2-increased attenuation of the bile because of the presence of intraductal debris,
3-diffuse and concentric bile duct wall thickening,
4-gas in the bile ducts or portal veins, and
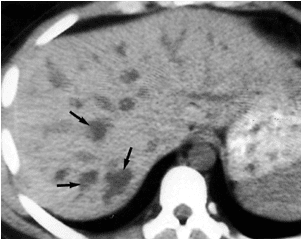
5- intrahepatic abscesses (seen as low-attenuation areas in contiguity with the intrahepatic bile ducts).
MRI can show a similar spectrum of findings (Fig. ). Because bile duct dilatation can be absent in patients with acute or partial obstruction, there is no correlation between the presence and degree of bile duct dilatation and the severity of acute cholangitis. However, the presence of hepatic abscesses, pneumobilia, and portal venous gas are indicative of a poor prognosis.
Reference:BiblioMed Textbook-Computed Body Tomography
























































{kind=link}