Transabdominal sonogram of an intrauterine pregnancy with marked oligohydramnios associated with intrauterine growth retardation. It is difficult to appreciate the fetal anatomy in the presence of oligohydramnios.

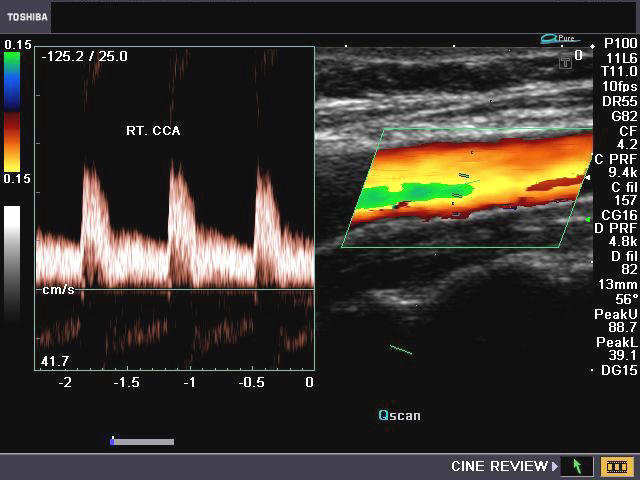
Normal spectral Doppler waveform of umbilical artery and vein in a near-term fetus.

Spectral Doppler waveform of umbilical artery in intrauterine growth retardation (IUGR) demonstrates loss of diastolic flow. Pulsatility of the umbilical vein can also be seen. Both of these findings suggest severe IUGR, and when seen, a perinatologist should be immediately informed.
Etiology
The causes of intrauterine growth retardation (intrauterine growth restriction; IUGR) can be either fetal or maternal
1-Fetal causes of IUGR include aneuploidy, trisomy 13, trisomy 18, triploidy, intrauterine infection, cytomegaloviral infection, and toxoplasmosis.
2-Maternal causes of IUGR include use of drugs (including recreational drugs such as marijuana), alcohol consumption, placental insufficiency, diabetes, late conception (possible cause), and a history of having a baby small for his or her age.
Asymmetrical vs symmetrical IUGR
In most cases of IUGR, especially those due to primary placental insufficiency, the fetal abdomen is small, but the head and extremities are normal or near normal. This finding is known as the head-sparing effect. In cases of severe, early-onset IUGR (those due to chromosomal anomalies), the fetus tends to be more symmetrically small. This condition leads to the existence of 2 distinct subgroups; however, these subgroups significantly overlap.
Sonographic criteria for IUGR
1-The sonographic criteria for IUGR include (1) an elevated ratio of femoral length to abdominal circumference (AC), (2) an elevated ratio of head circumference (HC) to AC, and (3) unexplained oligohydramnios.
2-The AC measurement is the best single measurement to assess fetal growth because, in growth curtailment, the liver is virtually always affected. Hadlock charts can be used to calculate the fetal weight from the AC.12 Most ultrasonography machines also use the Hadlock method of calculating fetal weight. The literature describes at least 47 formulas for the estimation of fetal weight. Using the Shepard formula (AC and biparietal diameter [BPD]), one can come within 5% of the true fetal weight and within 10% of the fetal weight 80% of the time. However, 20% of the time, the estimation of the fetal weight may be discrepant by more than 10%.
3-Oligohydramnios is an indicator of IUGR. Amniotic fluid of less than 5 cm, as measured in the four quadrants, is suggestive of oligohydramnios. Other causes of oligohydramnios include death in utero, renal agenesis, and premature rupture of membranes.
4-Abnormal findings on Doppler waveforms include the following:
-Highest uterine artery PI – lowest uterine artery PI greater than 1.1
- Persistence of protodiastolic notch, unilateral or bilateral, after 23 weeks is suggestive of IUGR or preeclampsia.
- RI greater than 0.55 with bilateral notches
- RI greater than 0.65 with a unilateral notch
-RI greater than 0.70 with or without notches
-RI greater than 90th percentile for a given gestational age regardless of notches
-An S/D ratio of greater than 3 after 30 weeks of gestation is abnormal.
-The reversal of flow in ductus venosus is suggestive of a fetus with severely compromised IUGR and reflects fetal metabolic acidemia.
5-Degree of Confidence
-Fetal weight below the 10th percentile has negative predictive value of 99%, a sensitivity of 89%, and a specificity of 88% for the detection of IUGR.
-An elevated HC-to-AC ratio has a negative predictive value of 98%, a sensitivity of 82%, and a specificity of 94% for the detection of IUGR.
-Decreased weight with decreased amniotic fluid and the presence of hypertension are good predictors of IUGR.








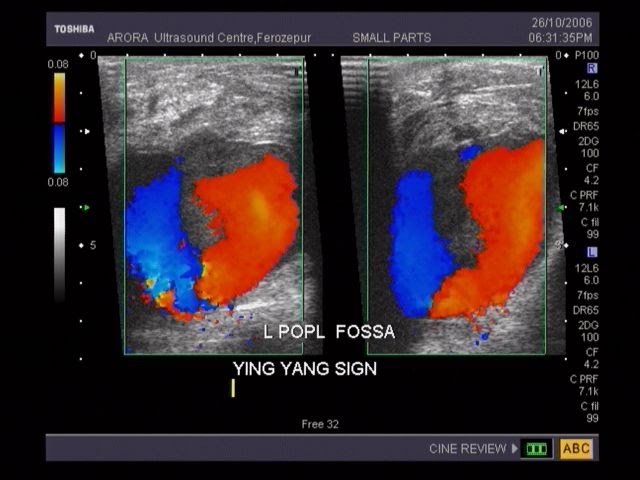
 This was a young adult male with complaint of small swelling in the left side of neck and mild dysphagia. On Color Doppler examination of the vessels of the neck, the right side showed normal diameter and flow in the right internal jugular vein and common carotid artery (see image on top left). However the left jugular vein showed a fusiform dilatation of the lower part of the vessel (close to its origin, ie: the proximal portion). Here, the vessel measured almost 12 to 14 mm. in diameter at rest. On deep inspiration and Valsalva maneuver, the rise in intrathoracic pressure resulted in diameter of the Internal jugular vein measuring 15 to 17 mm. (see image at bottom left). Compared to the the IJV on the right side the left IJV (internal jugular vein) also showed marked turbulence of flow both on Color Doppler imaging (see images on bottom left) and spectral Doppler waveform. The ultrasound/ Color Doppler images/ findings suggest Ectasia of the left Internal Jugular vein.
This was a young adult male with complaint of small swelling in the left side of neck and mild dysphagia. On Color Doppler examination of the vessels of the neck, the right side showed normal diameter and flow in the right internal jugular vein and common carotid artery (see image on top left). However the left jugular vein showed a fusiform dilatation of the lower part of the vessel (close to its origin, ie: the proximal portion). Here, the vessel measured almost 12 to 14 mm. in diameter at rest. On deep inspiration and Valsalva maneuver, the rise in intrathoracic pressure resulted in diameter of the Internal jugular vein measuring 15 to 17 mm. (see image at bottom left). Compared to the the IJV on the right side the left IJV (internal jugular vein) also showed marked turbulence of flow both on Color Doppler imaging (see images on bottom left) and spectral Doppler waveform. The ultrasound/ Color Doppler images/ findings suggest Ectasia of the left Internal Jugular vein. 































































{kind=link}
{kind=link}