 1-Anatomy
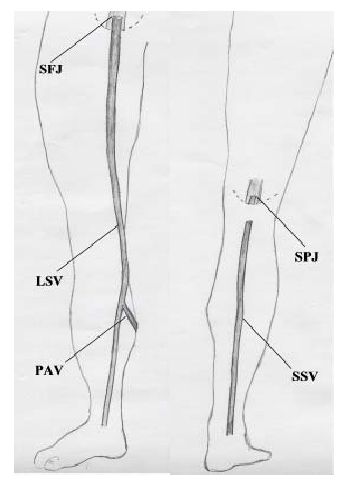
1-AnatomyThe superficial veins lie in the subcutaneous fatty layer of the body just beneath the skin and superficial to the deep fascia enveloping the body musculature. The principal veins in the legs are the great and lesser saphenous veins and their tributaries; in the arms they are the basilic and cephalic veins and their tributaries. The deep veins accompany arteries and bear the same name as the arteries they parallel. It is common in the extremities for there to be two or more veins accompanying a small- to medium-sized artery. The perforating veins penetrate the deep fascia and connect the superficial veins to the deep veins. Those along the inner (medial) side of the lower leg play a major role in the pathogenesis of the "postphlebitic leg". The intra-muscular sinusoidal veins are large, very thin walled, valveless veins within skeletal muscle. They connect directly with the deep veins.
 2-Physiology
2-PhysiologyThe venous system of vessels conducts blood back to the heart. Normal venous flow is dependent on four factors: the heart (dynamics/spontaneous flow), respiration (phasic flow), the venous pump and the valves.
Dynamic Flow: Flow in the arterial system is dependent on the pumping action of the heart and the elasticity and muscular activity of the arteries. In contrast, the veins, except for the major superficial veins, are thin walled with paucity of muscle; are designed for distention; and play an insignificant role in directly facilitating flow. Most of the force of the pulsatile flow produced by the pumping heart is lost as blood flows from the arteries through the vast network of capillaries (one cell layer micro-vessels where selective permeability allows the exchange of O2 and nutrients with the tissues). What pulsatile flow filters through (dynamic flow) is of low pressure (15mmHg). Nevertheless, it is sufficient to produce a significant pressure gradient with the right side of the heart where the venous pressure is 0.
Phasic Flow: is the effect of respiration on normal venous flow. In the arms and neck, flow towards the heart increases during inspiration due to the negative intra-thoracic pressure produced. The opposite is true in the legs. With inspiration the diaphragm descends increasing intra-abdominal pressure slowing flow. Flow is somewhat increased with expiration with reduced intra-abdominal pressure.
The "Muscle Pump": the muscle pump mechanism is most highly developed in the calf muscles. Large venous sinusoids located in these muscles act as a bellows and the contracting muscle the force emptying the bellows. Contractions of the calf muscles can produce a pressure in excess of 200 mmHg. This is sufficient pressure to empty the blood out of the sinusoids into the deep veins. The deep veins in turn are subject to a similar compressing force because of the strong fascial investment about the muscle compartment in which they are contained. As a result blood is pumped towards the heart with each muscle contraction (diagram #3).
Valves: valves are structured so that flow is always towards the heart and flow from superficial to deep veins. Without valves there would be one continuous column of blood from heart to ankle when an individual stood. By preventing reflux the valves complement the muscle pump in returning blood to the heart.
 3-pathology
3-pathologyThe most common pathological conditions in the venous system occur in the legs, and include valve incompetence and venous obstruction.
Venous obstruction is most commonly due to venous thrombosis, but may also result from vein compression (tumors, cervical rib, fractures, hematomas, arterial aneurysms etc). Factors producing venous thrombosis are vein injury, flow stasis (inactive muscle pump from lack of motion, bed confinement or paralysis), blood hypercoagulability (in post operative patient or an intrinsic coagulation disorder) and a combination of above as may occur in multiple trauma patients.
Valve incompetence may be due to congenital valve defect or develop as a complication of venous thrombosis and venous hypertension. Congenital valve incompetence occurs in the superficial veins and the perforators. Deep vein valve incompetence is considered a complication of previous deep vein thrombosis regardless that a history of deep vein thrombosis is obtained in less than 50% of patients.
Incompetence results in reflux with increased venous pressure in the segment of vein(s) below the incompetent valves when the individual stands (a condition referred to as "venous insufficiency"). Clinical manifestations depend on which venous system(s) (superficial, deep or perforators) are involved and the number of valves incompetent. When the valves of the deep veins are affected the ensuing venous hypertension produces backpressure in the capillaries causing leakage of fluid into the tissues with leg edema (swelling).
4-Venous Diseases
a-Varicose Veins
A varicose vein is dilated, elongated and tortuous. Most commonly affected are the saphenous veins in the legs (90% involve great saphenous system). The cause is venous hypertension resulting from valve incompetence. They may be primary or secondary.
Primary (saphenous) varicose veins
This is a congenital condition. Varices result from congenital weakness of the valve structure and possibly also a congenital weakness in the vein wall. There is a family history in 75% of patients. By themselves primary varicose veins produce few symptoms. Cosmetic appearance is the major complaint. A common symptom is heaviness of the legs towards the end of the day, particularly for those whose occupation requires considerable walking and standing. There should be little to no ankle or leg swelling.
Secondary Varicose Veins
Secondary varices are a sequela of either deep vein obstruction, incompetent deep vein valves or a combination of both. In each case the resulting venous hypertension renders the perforating veins incompetent allowing unrestricted back flow from deep to superficial veins. The superficial veins not being structured to withstand a high venous pressure become dilated and elongated, forming secondary varices.
Thrombophlebitis, Venous Thrombosis
When a thrombus (blood clot) obstructs a vein it sets up a sterile inflammatory reaction in the vein wall and the surrounding tissue. This condition is known as "thrombophlebitis". When a loosely attached thrombus develops in a vein and is not obstructing, it produces no reaction in the vein wall. This condition is known as "phlebothrombosis."
Superficial Thrombophlebitis:
Superficial thrombophlebitis of the great saphenous vein presents with a typical clinical picture. It begins with sudden development of pain and tenderness along the course of the section of vein involved. The skin over the vein is red and the adjacent tissue swollen. With resolution of the inflammation (2-3 weeks if untreated) the thrombosed vein can be felt as a cord-like structure beneath the skin.
The cause of the phlebitis and the reason that the great saphenous vein is usually targeted remains unknown. Local trauma and/or unusual activity may be a precipitating cause in some cases. It can be recurrent, developing in another section of the saphenous vein in the same leg. Superficial phlebitis is more of an annoyance than a serious condition. It resolves rapidly with reduced activity and anti-inflammatory drugs. However, in those cases where the thrombotic process extends to the level of the groin, there is a risk of involvement of the common femoral vein and the possibility of pulmonary embolism.
Superficial saphenous vein thrombophlebitis is distinct from thrombosis occurring in a cluster of varices. The latter is common in varicose vein disease. There is no risk of pulmonary embolism. Permanent discolouration of the overlying skin is the main complication. In the arms the common cause of superficial phlebitis is chemical damage to the lining of the vein from intravenous injection. Pulmonary embolism secondary to thrombophlebitis in the arms is rare.
Deep venous thrombosis (D.V.T)
D.V.T. by medical convention refers to thrombosis in the deep veins of the legs. It is a relatively common complication of major surgery, leg fractures and prolonged bed rest. Stasis because of muscle pump inactivity, a hypercoagulable state which is a biological reaction to injury and, local trauma to veins, all play a role.
The clinical presentation is related to site, extent and degree of obstruction produced by the thrombus. Thrombosis limited to the calf veins produces only mild calf soreness and tenderness and minimal, if any, ankle swelling. In contrast acute thrombosis obstructing the femoral and iliac veins results in a grossly swollen, painful, white leg (white because of the extensive edema under the skin). Rarely the extent of the thrombosis will include the entire venous network causing obstruction of arterial circulation. The result is massive leg swelling complicated by manifestations of vascular ischemia and possible gangrene (so called venous gangrene). When deep vein thrombosis does not cause obstruction (i.e. phlebothrombosis) pulmonary embolism may be the first and only clinical manifestation.
Acute D.V.T. is a medical emergency. Anticoagulation (blood thinning) is the prime treatment. It prevents extension of the thrombus. Clot lysing drugs (thrombokinins) are injected transvenously in selected cases. Thrombectomy (surgical removal of clot) has a limited role.
Recurrence of acute D.V.T. is common. Major complications include pulmonary embolism, chronic deep vein insufficiency and the postphlebitic leg.
Pulmonary Embolism
Pulmonary embolism occurs when a piece of clot (thrombus) breaks away from the vein wall, enters the venous flow and passes through the right side of the heart to lodge in the pulmonary artery or one of its branches. Clinical manifestations are determined by the size of the clot and the size of the vessel occluded. The spectrum includes sudden death (occlusion of main pulmonary artery), pleurisy-like symptoms from lung infarction (occlusion of segmental artery and local lung death); shortness of breath and pulmonary insufficiency (occlusion of multiple small vessels from showers of small emboli). Acute D.V.T. is the major source of pulmonary embolism.
Lung scans and pulmonary angiograms confirm the diagnosis. Immediate and full anticoagulation (blood thinning) is basic treatment. Where obstruction of the main pulmonary or major branch is diagnosed thrombolytic agents are injected directly into the clot by intravenous catheter. Surgical removal of the blood clots is warranted in selected cases. When the use of anticoagulants, is contraindicated a filter is inserted into the inferior vena cava to prevent further clots from reaching the lung.
Chronic Venous Insufficiency and Postphlebtic Leg
Chronic venous insufficiency is an overarching term which includes the various clinical and pathological entities resulting from impaired venous flow and venous hypertension. Chronic venous insufficiency in the deep veins is attributable to acute D.V.T. and its sequelae. The degree of insufficiency initially depends on the fate of the obstructing thrombus. The thrombus may be partially or completely dissolved by lytic enzymes. More commonly it is organized and replaced by fibrous tissue with varying degrees of recanalization (the development of small, valveless channels traversing the length of the organized thrombus). Recanalization produces little improvement in venous flow. Compensatory dilatation of collateral veins (superficial and deep secondary veins which bypass the obstructed area) is more effective in re-establishing the venous flow. The dilated superficial veins which may result are referred to as secondary varicose veins.
D.V.T. has a disastrous effect on the valves of the deep and perforating veins partially due to injury to the valves by the process of thrombosis, and more particularly due to venous hypertension, which produces abnormal dilatation of both the deep and perforating veins rendering their valves incompetent. The result is the inability of the venous pump to provide relief from venous hypertension when the individual stands and walks. As a consequence, the capillaries in the distal part of the legs are exposed to a high pressure (Diagram #4).
The result is increased capillary permeability with leakage of fluids into the tissues producing leg edema (swelling). The concentration of perforators around the ankle and the higher hydrostatic pressure with standing makes this area (the so-called "gaiter area") particularly vulnerable. Diagram 5









































































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}