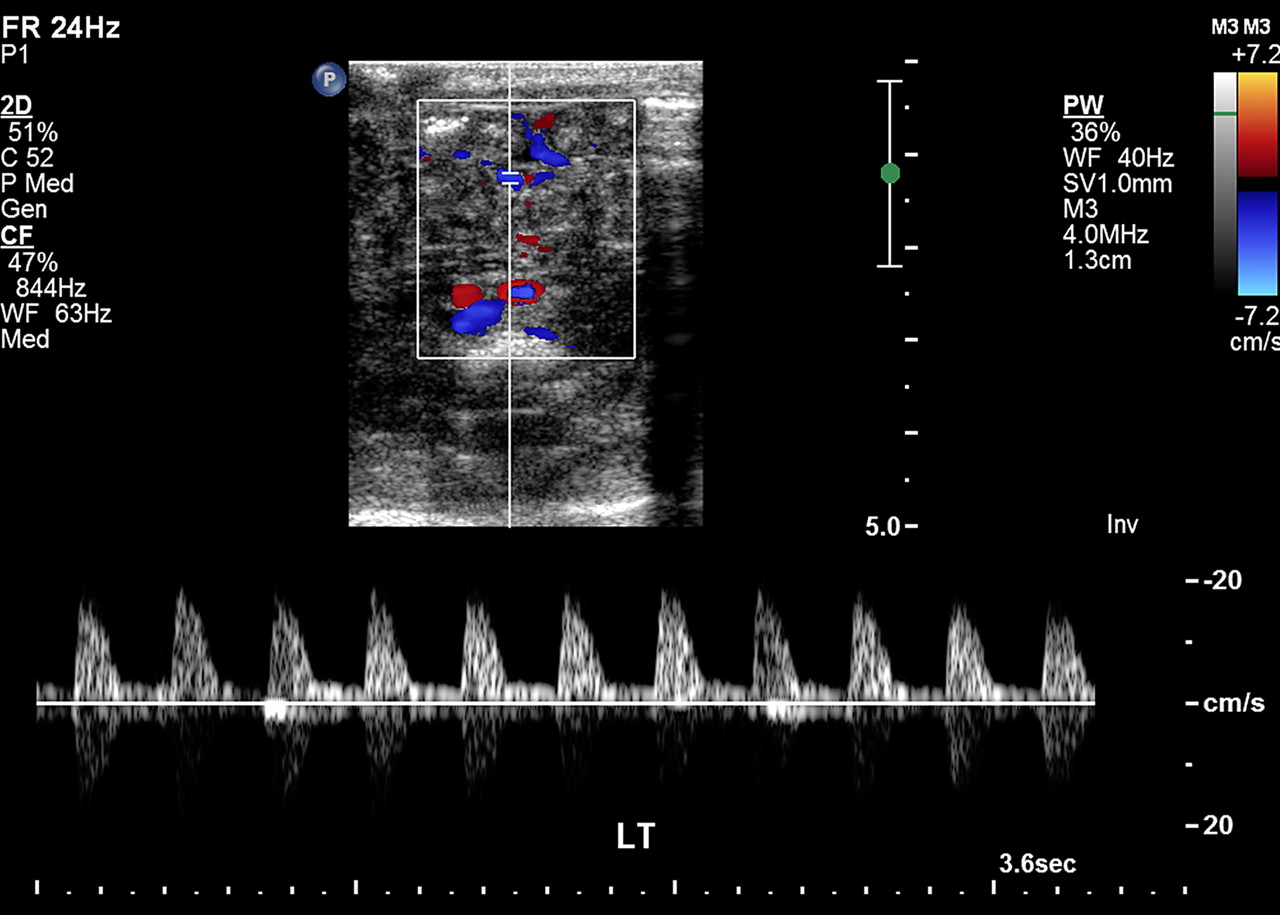
Normal spectral waveforms from lower limb veins. (a) Common femoral vein waveform obtained during breath holding in an 11-year-old boy shows a, S, v, and D waves. (b) Waveform from the popliteal vein in an 11-year-old boy shows a reduced flow velocity during inspiration and an increased velocity during expiration. (c) Posterior tibial vein waveform from an 11-year-old boy shows phasic variations from respiration with mild superimposed undulation from right atrial pressure changes.
Normal spectral waveforms from lower limb veins. (a) Common femoral vein waveform obtained during breath holding in an 11-year-old boy shows a, S, v, and D waves. (b) Waveform from the popliteal vein in an 11-year-old boy shows a reduced flow velocity during inspiration and an increased velocity during expiration. (c) Posterior tibial vein waveform from an 11-year-old boy shows phasic variations from respiration with mild superimposed undulation from right atrial pressure changes. The phasic pattern of flow in lower limb veins reflects a combination of both cardiac and respiratory movements (3). Normally, all four waves that represent right atrial changes can be seen in the spectral line (Fig 10). If the S, v, and D waves are completely above the baseline and the a wave is either completely above the baseline or descends less than 5 cm/sec below it, normal antegrade flow is considered to be present. A deeper descent of the a wave below the baseline is indicative of retrograde or pulsatile flow, a pattern suggestive of increased right atrial pressure (12).
During inspiration, increased intraabdominal pressure results in a reduction of venous return from the lower limbs, which in turn leads to a decrease in the velocity or amplitude of the waveform. During expiration, flow velocities in the lower limb veins increase (3). The maximum flow velocity in femoral veins in adults is 12–30 cm/sec (13).