
1-use linear array probe 5 - 7.5 mhz.
2-patient supine with slight abduction of the thigh 10-15 degree.
3-gel applied from groin to adductor canal.
4-first,imaging done in transverse plane to identify femoral vein(medial) and artery(lateral).
5-spectral doppler analysis of both vessels.
artery--->triphasic wave form.
vein --->monophasic wave form.
6-examine external iliac vein using spectral wave form by one or the two following
a - normally , it is monophasic wave form with increase with expiration and decrease with inspiration.
-absence of this variation means----->proximal thrombosis or
----->proximal compression of the vein.
b-by valsalva maneuver.
7-by this point,imaging will be done by longitudinal scan.
8-examination of--->common femoral vein.
--->superficial femoral vein.
--->profunda femoris vein.
we can increase doppler flow by--->compression technique
and by--->by power doppler imaging.
8-turn patient in lateral decubitus with knee flexed by 20-25 degrees.
9-popliteal vein is seen anterior to popliteal artery.
10-examine popliteal vein up to adductor canal and inferiorly to tibio-peroneal trunk.
11-diagnostic criteria
*sponteneous flow:
present in patent vessel
not present in thrombotic vessel.
*intraluminal reflective material:
not present in patent vessel.
present in thrombotic vessel.
*response to distal augmentation:
present in patent vessel.
not present in thrombotic vessel.
*response to probe compression:
present in patent vessel.
not present in thrombotic vessel.
*venous dilatation:
not present in patent vessel.
present in thrombotic vessel.
*spectral wave form:
present,phasic in patent vessel.
not present in thrombotic vessel.
iliac assessment:
spectral variation is seen in patent vessel.
not seen in thrombotic vessel.
response to valsalva maneuver is seen in healthy vein
not present in thrombotic vessel.
Saturday, August 14, 2010
real time compression ultrasound
1- put the probe perpendicular to the vascular flow.
2-start at groin.
3-identify common femoral vein(medial) and artery(lateral).
4-use linear array probe 5-7.5 mhz.
5-make a light pressure so the vein will not be closed.
6-then put further pressure on the vein
if it is collapsed completely(both walls opposed to each other)---> it is a healthy vein
if it is not collapsed at all or collapsed partially---> vein contains thrombus.
7-reflective thrombus could be seen within the lumen of the vein.
8-apply this technique from the groin to the adductor canal with 1 cm intervals.
9-to examine the popliteal vein turn the patient into lateral decubitus position with knee flexed.
10-then from posterior fossa , the vein will be anterior to the artery.
11-popliteal vein is followed upward to adductor canal and inferiorly to tibio-peroneal trunk.
12-at this point , examination was ended.
2-start at groin.
3-identify common femoral vein(medial) and artery(lateral).
4-use linear array probe 5-7.5 mhz.
5-make a light pressure so the vein will not be closed.
6-then put further pressure on the vein
if it is collapsed completely(both walls opposed to each other)---> it is a healthy vein
if it is not collapsed at all or collapsed partially---> vein contains thrombus.
7-reflective thrombus could be seen within the lumen of the vein.
8-apply this technique from the groin to the adductor canal with 1 cm intervals.
9-to examine the popliteal vein turn the patient into lateral decubitus position with knee flexed.
10-then from posterior fossa , the vein will be anterior to the artery.
11-popliteal vein is followed upward to adductor canal and inferiorly to tibio-peroneal trunk.
12-at this point , examination was ended.
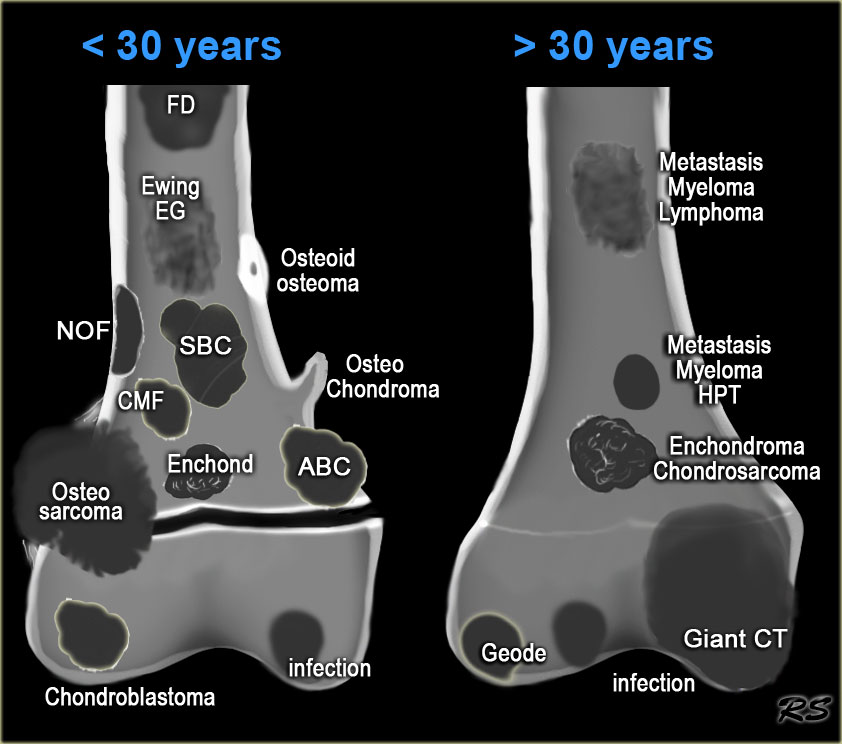
In the article Bone Tumors - Differential diagnosis we discuss a systematic approach to the differential diagnosis of bone tumors and tumor-like lesions. In this article we will discuss the differential diagnosis of well-defined osteolytic bone tumors and tumor-like lesions.
Abbreviations used:
-ABC = Aneurysmal bone cyst
-CMF = Chondromyxoid fibroma
-EG = Eosinophilic Granuloma
- GCT = Giant cell tumour
-FD = Fibrous dysplasia
- HPT = Hyperparathyroidism with Brown tumor
-NOF = Non Ossifying Fibroma SBC = Simple Bone Cyst
http://www.radiologyassistant.nl/en/4bc6176e56228
Abbreviations used:
-ABC = Aneurysmal bone cyst
-CMF = Chondromyxoid fibroma
-EG = Eosinophilic Granuloma
- GCT = Giant cell tumour
-FD = Fibrous dysplasia
- HPT = Hyperparathyroidism with Brown tumor
-NOF = Non Ossifying Fibroma SBC = Simple Bone Cyst
http://www.radiologyassistant.nl/en/4bc6176e56228
 On the above the most common well-defined bone tumors and tumor-like lesions.These lesions are sometimes referred to as benign cystic lesions, which is a misnomer since most of them are not cystic, except for SBC and ABC. It is true that in patients under 30 years a well-defined border means that we are dealing with a benign lesion, but in patients over 40 years metastases and multiple myeloma have to be included in the differential diagnosis
On the above the most common well-defined bone tumors and tumor-like lesions.These lesions are sometimes referred to as benign cystic lesions, which is a misnomer since most of them are not cystic, except for SBC and ABC. It is true that in patients under 30 years a well-defined border means that we are dealing with a benign lesion, but in patients over 40 years metastases and multiple myeloma have to be included in the differential diagnosishttp://www.radiologyassistant.nl/en/4bc6176e56228

On the above a table with well-defined osteolytic bone tumors and tumor-like lesions in different age-groups.
-Notice the following:
-In patients <>
-In patients > 40 years metastases and multiple myeloma are by far the most common well-defined osteolytic bone tumors.
- Patients with Brown tumor in hyperparathyroidism should have other signs of HPT or be on dialysis.
-Differentiation between a benign enchondroma and a low grade chondrosarcoma can be impossible based on imaging findings only.
- Infection is seen in all ages.
 - Most bone tumors present as well-defined osteolytic lesions, sometimes referred to as 'bubbly lesions'.
- Most bone tumors present as well-defined osteolytic lesions, sometimes referred to as 'bubbly lesions'.-It is important to have a good differential diagnostic approach to these lesions.
-You can use the table above, but another way to look at the differential diagnosis of well defined osteolytic bone lesions is to use the mnemonic Fegnomashic, which is popularized by Clyde Helms (1).
-Some prefer to use the mnemonic Fogmachines, which is formed by the same letters, but is a real word.
http://www.radiologyassistant.nl/en/4bc6176e56228
Fibrous Dysplasia

Fibrous dysplasia
-Fibrous dysplasia is a benign disorder characterized by tumor-like proliferation of fibro-osseus tissue and can look like anything.
-FD most commonly presents as a long lesion in a long bone.
-FD is often purely lytic and takes on ground-glass look as the matrix calcifies.
-In many cases there is bone expansion and bone deformity.
-The ipsilateral proximal femur is invariably affected when the pelvis is involved.
-When FD in the tibia is considered, adamantinoma should be in the differential diagnosis. Discriminator:
If periosteal reaction or pain is present, exclude fibrous dysplasia, unless there is a fracture.
http://www.radiologyassistant.nl/en/4bc6176e56228
Enchondroma
 • left
• leftFat suppressed coronal PD-image of the knee. Typical enchondromas in the femur and tibia as seen frequently as coincidental finding in MR-examinations.
middle
Well-defined lytic lesion in the rib with cortical thinning.
right
Well-defined lytic lesion with a sclerotic margin and without calcifications in the end phalanx.
Enchondroma
 Enchondroma
Enchondroma-Enchondroma is a benign cartilage tumor.
-Frequently it is a coincidental finding.
-In the phalanges of the hand it frequently presents with a fracture.
-It is the most common lesion in the phalanges, i.e. a well-defined lytic lesion in the hand is almost always an enchondroma.
-In some locations it can be difficult to differentiate between enchondroma and bone infarct.
-It is almost impossible to differentiate between enchondroma and low grade chondrosarcoma based on radiographic features alone.
-Ollier's disease is multiple enchondromas.
-Maffucci's syndrome is multiple enchondromas with soft tissue hemangiomas.
-Features that favor the diagnosis of a low-grade chondrosarcoma:
Higher age Size > 5 cm
Activity on bone scan
Fast enhancement on dynamic contrast enhanced MR series
Endosteal scalloping of the cortical bone
Discriminators :
Must have calcification except in phalanges.
No periostitis.
http://www.radiologyassistant.nl/en/4bc6176e56228

EG
- is a non-neoplastic proliferation of histiocytes and is also known as Langerhans cell histiocytosis.
-It should be included in the differential diagnosis of any sclerotic or osteolytic lesion, either well-defined or ill-defined, in patients under the age of 30.
-The diagnosis EG can be excluded in age > 30.
-EG is usually monostotic, but can be polyostotic.
- left
Osteolytic lesion arising from the neurocranium with associated soft tissue swelling.
middle
Mixed lytic-sclerotic lesion, not well-defined with solid periosteal reaction.
right
Sharply defined osteolytic lesion of the skull. There is no 'button sequestrum', which is more or less pathognomonic.Discriminator: Must be under age 30.
giant cell tumor
 Giant cell tumor
Giant cell tumor-Giant cell tumor is a lesion with multinucleated giant cells.
-In most cases it is a benign lesion.
-Malignant GCT is rare and differentiation between benign or malignant GCT is not possible based on the radiographs.
-GCT is also included in the differential diagnosis of an ill-defined osteolytic lesion, provided the age and the site of the lesion are compatible.
-Discriminators:
Epiphyses must be closed.
Must be an epiphyseal lesion and abut the articular surface.
Must be well-defined and non-sclerotic margin. Must be eccentric.
http://www.radiologyassistant.nl/en/4bc6176e56228
 NOF: typical presentation as an eccentric, multi-loculated subcortical lesion with a central lucency and a scalloped sclerotic margin.
NOF: typical presentation as an eccentric, multi-loculated subcortical lesion with a central lucency and a scalloped sclerotic margin.NOF
-NOF is a benign well-defined, solitary lesion due to proliferation of fibrous tissue.
-It is the most common bone lesion.
-NOF is frequently a coincidental finding with or without a fracture.
-NOF usually has a sclerotic border and can be expansile.
-They regress spontaneously with gradual fill in.
-NOF may occur as a multifocal lesion. The radiographic appearance is almost always typical, and as such additional imaging and biopsy is not warranted.
Discriminators:
Must be under age 30.
No periostitis or pain.
http://www.radiologyassistant.nl/en/4bc6176e56228
osteoblastoma
 Osteoblastoma
Osteoblastoma-Osteoblastoma is a rare solitary, benign tumor that produces osteoid and bone.
-Consider osteoblastoma when ABC is in the differential diagnosis of a spine lesion (figure).
-A typical osteoblastoma is larger than 2 cm, otherwise it completely resembles osteoid osteoma. Discriminator: Mention when ABC is mentioned.
http://www.radiologyassistant.nl/en/4bc6176e56228
bone metastases
 Metastases
Metastases-Metastases are the most common malignant bone tumors.
-Metastases must be included in the differential diagnosis of any bone lesion, whether well-defined or ill-defined osteolytic or sclerotic in age > 40.
-Bone metastases have a predilection for hematopoietic marrow sites: spine, pelvis, ribs, cranium and proximal long bones: femur, humerus.
-Metastases can be included in the differential diagnosis if a younger patient is known to have a malignancy, like neuroblastoma, rhabdomyosarcoma, retinoblastoma.
-Most common osteolytic metastases: kidney, lung, colon and melanoma.
-Most common osteosclerotic metastases: prostate and breast.
Discriminator: Must be over age 40.
http://www.radiologyassistant.nl/en/4bc6176e56228
multiple myeloma
 Multiple Myeloma
Multiple Myeloma-Multiple myeloma must be included in the differential diagnosis of any lytic bone lesion, whether well-defined or ill-defined in age > 40.
-The most common location is in the axial skeleton (spine, skull, pelvis and ribs) and in the diaphysis of long bones (femur and humerus).
-Most common presentation: multiple lytic 'punched out' lesions.
-Multiple myeloma doe not show any uptake on bone scan.
-Discriminator: Must be over age 40.
http://www.radiologyassistant.nl/en/4bc6176e56228
multiple myeloma
 Multiple Myeloma (2)
Multiple Myeloma (2)Differential diagnosis:
multiple lesions: metastases.
solitary lesion: chondrotumor, GCT and lymphoma.
- On the above a CT-image of a patient with multiple myeloma.Notice the numerous osteolytic lesions and permeative cortical destruction pattern.
In the left sacral wing there is a larger lesion with a high density due to replacement of fatty bone marrow by myeloma (red arrow).
http://www.radiologyassistant.nl/en/4bc6176e56228
 SBC: well-defined osteolytic lesion without expansion of the proximal meta-diaphysis of the humerus with pathologic fracture
SBC: well-defined osteolytic lesion without expansion of the proximal meta-diaphysis of the humerus with pathologic fractureSolitary Bone Cyst
-Solitary bone cyst, also known as unicameral bone cyst, is a true cyst.
- Many well-defined osteolytic lesions are often called cystic, but this is a misnomer.
-SBC frequently presents with a fracture. Sometimes a fallen fragment is appreciated. Predilection sites: proximal humerus and femur.
-Usually less expansion compared with ABC.
-Differential diagnosis: ABC, FD when cystic. SBC may migrate from metaphysis to diaphysis during growth of the bone.
-Discriminators:
Must be under age 30.
Must be centric
http://www.radiologyassistant.nl/en/4bc6176e56228

Hyperparathyroidism
-Brown tumors can occur in any bone and present as osteolytic lesions with sharp margins. Septa and ridges may be seen.
-Differential diagnosis: ABC, metastases and GCT depending on location and age.
-On the above a patient who had a nefrectomy for renal cell carcinoma and who was on dialysis. Multiple well-defined osteolytic lesions were found on a follow up CT scan.
-The differential diagnosis included metastases and Brown tumors in hyperparathyroidism. Biopsy revealed Brown tumor.
-Discriminators: Must have other signs of HPT.
http://www.radiologyassistant.nl/en/4bc6176e56228
 Infection
Infection-Infection or osteomyelitis is the great mimicker of bone tumors.
-It has a broad spectrum of radiographic features and occurs at any age and has no typical location.
-In the chronic stage it can mimic a benign bone tumor (Brodies abscess).
-In the acute stage it can mimic a malignant bone tumor with ill-defined margins, cortical destruction and an aggressive type of periostitis.
-Only when there is a thick solid periosteal reaction we can recognize the non-malignant underlying process
-Discriminators:
None.
http://www.radiologyassistant.nl/en/4bc6176e56228
 Chondroblastoma: notice extensive edema (middle) and fluid-fluid level due to secondary ABC.
Chondroblastoma: notice extensive edema (middle) and fluid-fluid level due to secondary ABC.
Chondroblastoma
-The patella, carpal and tarsal bones can be regarded as epiphysis conceirning.
- the differential diagnosis.
- On the above a chondroblastoma located in the patella.Discriminators :
- must be under age 30.
-must be in the epiphysis.
 Chondromyxoid Fibroma
Chondromyxoid Fibroma-Chondromyxoid Fibroma is a rare lesion.
-CMF resembles NOF.
-Preferential sites: proximal tibia and foot.
- Although the name suggests that CMF is a chondroid lesion, calcifications are usually not seen. On the above images of a CMF.
- There is an eccentric osteolytic lesion in the metaphysis of the proximal tibia. On the inner side there is a sclerotic margin. On the outer side there is a regular cortical destruction with peripheral bone layer.
-The MR also shows a sclerotic margin with low signal intensity
-Discriminators : Mention when an NOF is mentioned.
Thursday, August 12, 2010

Wednesday, August 11, 2010
Deep vein thrombosis: scintigraphic diagnosis with In-111-labeled monoclonal antifibrin antibodies.
1-Fifty-two patients suspected of having deep vein thrombosis under-went scintigraphy with an indium-111-labeled monoclonal antifibrin antibody.
2- Venography disclosed deep vein thrombosis in 31 patients.
3-With the whole limb considered an anatomic entity, antifibrin antibody scintigrams obtained 2 hours after injection had a specificity and sensitivity of 81% and 84%, respectively.
4-A higher sensitivity (92%) was found for a subgroup of patients (n = 44) with symptoms for less than 10 days.
5-Regional sensitivities for all patients and for the subgroup, respectively, were 92% and 100% in the calf, 82% and 94% in the popliteal region, 63% and 71% in the thigh, and only 18% and 13% in the pelvis. Additional imaging performed 6 hours and 21 hours after injection in 12 patients and quantitative analysis done from scintigrams with and without blood-pool (technetium-99m human serum albumin) correction did not improve sensitivity. In-111-antifibrin antibody scintigraphy is an accurate method for diagnosis of acute established deep vein thrombosis of the calf and popliteal region; its sensitivity in the thigh is lower, and it is not feasible for diagnosis in the pelvic area.
http://www.ncbi.nlm.nih.gov/pubmed/2678259
2- Venography disclosed deep vein thrombosis in 31 patients.
3-With the whole limb considered an anatomic entity, antifibrin antibody scintigrams obtained 2 hours after injection had a specificity and sensitivity of 81% and 84%, respectively.
4-A higher sensitivity (92%) was found for a subgroup of patients (n = 44) with symptoms for less than 10 days.
5-Regional sensitivities for all patients and for the subgroup, respectively, were 92% and 100% in the calf, 82% and 94% in the popliteal region, 63% and 71% in the thigh, and only 18% and 13% in the pelvis. Additional imaging performed 6 hours and 21 hours after injection in 12 patients and quantitative analysis done from scintigrams with and without blood-pool (technetium-99m human serum albumin) correction did not improve sensitivity. In-111-antifibrin antibody scintigraphy is an accurate method for diagnosis of acute established deep vein thrombosis of the calf and popliteal region; its sensitivity in the thigh is lower, and it is not feasible for diagnosis in the pelvic area.
http://www.ncbi.nlm.nih.gov/pubmed/2678259
Antifibrin scintigraphy in the diagnostic evaluation of acute deep venous thrombosis
1-Antifibrin scintigraphy is a new and innovative approach to the diagnosis of acute deep venous thrombosis (DVT).
2-Many antifibrin monoclonal antibodies (Mo-Abs) have been described, but only two, 59D8 and T2G1s, have undergone broad preclinical or clinical investigation. Both of these MoAbs recognize an epitope on the amino terminal end of fibrin. The epitope for 59D8 and T2G1s is available for binding only on newly formed, acute thrombi.
3-Preclinical studies have confirmed the specificity of these MoAbs for acute DVT, and have demonstrated their ability to image experimentally induced DVT.
4- Preliminary clinical studies in patients with signs or symptoms of DVT have evaluated indium-111 59D8 Fab and technetium-99m T2G1s Fab'. Fragments of the intact MoAbs are employed to promote faster blood clearance and to reduce immunogenicity.
5-The initial clinical studies indicate that antifibrin scintigraphy has a diagnostic accuracy approaching 90%.
6-Antifibrin scintigraphy has the potential for overcoming many of the deficiencies of both invasive (contrast venography) and noninvasive (Doppler/ultrasound, impedance plethysmography) methods for detecting DVT. With a single procedure, it provides an accurate and rapid evaluation of both lower extremities, both above and below the knee. Because of its unique specificity for acute DVT, it should have excellent potential for use in patients with suspected acute, recurrent DVT, a condition difficult to diagnose by all currently employed tests for DVT.
http://www.seminarsinnuclearmedicine.com/article/S0001-2998(05)80134-5/abstract
2-Many antifibrin monoclonal antibodies (Mo-Abs) have been described, but only two, 59D8 and T2G1s, have undergone broad preclinical or clinical investigation. Both of these MoAbs recognize an epitope on the amino terminal end of fibrin. The epitope for 59D8 and T2G1s is available for binding only on newly formed, acute thrombi.
3-Preclinical studies have confirmed the specificity of these MoAbs for acute DVT, and have demonstrated their ability to image experimentally induced DVT.
4- Preliminary clinical studies in patients with signs or symptoms of DVT have evaluated indium-111 59D8 Fab and technetium-99m T2G1s Fab'. Fragments of the intact MoAbs are employed to promote faster blood clearance and to reduce immunogenicity.
5-The initial clinical studies indicate that antifibrin scintigraphy has a diagnostic accuracy approaching 90%.
6-Antifibrin scintigraphy has the potential for overcoming many of the deficiencies of both invasive (contrast venography) and noninvasive (Doppler/ultrasound, impedance plethysmography) methods for detecting DVT. With a single procedure, it provides an accurate and rapid evaluation of both lower extremities, both above and below the knee. Because of its unique specificity for acute DVT, it should have excellent potential for use in patients with suspected acute, recurrent DVT, a condition difficult to diagnose by all currently employed tests for DVT.
http://www.seminarsinnuclearmedicine.com/article/S0001-2998(05)80134-5/abstract
Tuesday, August 10, 2010
Abbreviations
Abbreviations used:
ABC = Aneurysmal bone cyst
CMF = Chondromyxoid fibroma
EG = Eosinophilic Granuloma
GCT = Giant cell tumour
FD = Fibrous dysplasia
HPT = Hyperparathyroidism with Brown tumor
NOF = Non Ossifying Fibroma SBC = Simple Bone Cyst
http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
ABC = Aneurysmal bone cyst
CMF = Chondromyxoid fibroma
EG = Eosinophilic Granuloma
GCT = Giant cell tumour
FD = Fibrous dysplasia
HPT = Hyperparathyroidism with Brown tumor
NOF = Non Ossifying Fibroma SBC = Simple Bone Cyst
http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15



Bone tumors in the spine
Bone tumors in the spine
 1- Hemangioma.
1- Hemangioma.
2-Metastasis.
3- Multiple myeloma.
4-Plasmocytoma: vertebra plana.
This 'Mini Brain' appearance of plasmacytoma in the spine is sufficiently pathognomonic to obviate biopsy .

http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
 1- Hemangioma.
1- Hemangioma.2-Metastasis.
3- Multiple myeloma.
4-Plasmocytoma: vertebra plana.
This 'Mini Brain' appearance of plasmacytoma in the spine is sufficiently pathognomonic to obviate biopsy .

http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
polyostotic lesions

Fig:Polyostotic Fibrous Dysplasia. Multiple osteolytic lesions in femur.
Polyostotic or multiple lesions
Most bone tumors are solitary lesions. If there are multiple or polyostotic lesions, the differential diagnosis must be adjusted.
Polyostotic lesions <> 30 years
Common: Metastases, multiple myeloma, multiple enchondromas.
Less common: Fibrous dysplasia, Brown tumors of hyperparathyroidism, bone infarcts.
Mnemonic for multiple oseolytic lesions: FEEMHI: Fibrous dysplasia, enchondromas, EG, Mets and myeloma, Hyperparathyroidism, Infection.
http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
osteoid matrix
 Osteoid matrix
Osteoid matrix-Mineralization in osteoid tumors can be described as a trabecular ossification pattern in benign bone-forming lesions and as a cloud-like or ill-defined amorphous pattern in osteosarcomas. Sclerosis can also be reactive, e.g. in Ewing sarcoma or lymphoma.
left
Cloud-like bone formation in osteosarcoma. Notice the aggressive, interrupted periosteal reaction (arrows).
right Trabecular ossification pattern in osteoid osteoma. Notice osteolytic nidus (arrow).
http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
chondroid matrix
 Matrix
Matrix-Calcifications or mineralization within a bone lesion may be an important clue in the differential diagnosis.
-There are two kinds of mineralization: a chondroid matrix in cartilaginous tumors like enchondromas and chondrosarcomsa and an osteoid matrix in osseus tumors like osteoid osteomas and osteosarcomas.
-Chondroid matrix
Calcifications in chondroid tumors have many descriptions: rings-and-arcs, popcorn, focal stippled or flocculent.
left: Enchondroma, the most commonly encountered lesion of the phalanges.
middle: middle: Peripheral chondrosarcoma, arising from an osteochondroma (exostosis).
right: Chondrosarcoma of the rib.
http://www.radiologyassistant.nl/en/494e15cbf0d8d#a4b331e94d0f15
Monday, August 9, 2010
Location: centric - eccentric - juxtacortical
 Location: centric - eccentric - juxtacortical
Location: centric - eccentric - juxtacortical-Centric in long bone
SBC, eosinophilic granuloma, fibrous dysplasia, ABC and enchondroma are lesions that are located centrally within long bones.
-Eccentric in long bone
Osteosarcoma, NOF, chondroblastoma, chondromyxoid fibroma, GCT and osteoblastoma are located eccentrically in long bones.
-CorticalOsteoid osteoma is located within the cortex and needs to be differentiated from osteomyelitis.
-JuxtacorticalOsteochondroma.
The cortex must extend into the stalk of the lesion.
-Parosteal osteosarcoma arises from the periosteum.
1-SBC:
central diaphyseal
2-NOF:
eccentric metaphyseal
3-SBC:
central diaphyseal
4-Osteoid osteoma:
cortical
5-Degenerative subchondral cyst: epiphyseal
6-ABC: centric diaphyseal
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Location: epiphysis - metaphysis - diaphysis
 Location: epiphysis - metaphysis - diaphysis
Location: epiphysis - metaphysis - diaphysis-Epiphysis
Only a few lesions are located in the epiphysis, so this could be an important finding.
1-In young patients it is likely to be either a chondroblastoma or an infection.
2-In patients over 20, a giant cell tumor has to be included in the differential diagnosis.
3-In older patients a geode, i.e. degenerative subchondral bone cyst must be added to the differential diagnosis.
4-Look carefully for any signs of arthrosis.
-Metaphysis
NOF, SBC, CMF, Osteosarcoma, Chondrosarcoma, Enchondroma and infections.
-Diaphysis
Ewing's sarcoma, SBC, ABC, Enchondroma, Fibrous dysplasia and Osteoblastoma.
-Differentiating between a diaphyseal and a metaphyseal location is not always possible. Many lesions can be located in both or move from the metaphysis to the diaphysis during growth.Large lesions tend to expand into both areas.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Location within the skeleton
 Location within the skeleton
Location within the skeletonThe location of a bone lesion within the skeleton can be a clue in the differential diagnosis. The above illustration shows the preferred locations of the most common bone tumors. In some locations, such as in the humerus or around the knee, almost all bone tumors may be found.
Top five location of bone tumors in alphabethic order
- Aneurysmal Bone Cyst
tibia, femur, fibula, spine, humerus
-Adamantinoma
tibia shaft, mandible
-Chondroblastoma
femur, humerus, tibia, tarsal bone (calc), patella
- Chondromyxoid fibroma
tibia, femur, tarsal bone, phalanx foot, fibula
-Chondrosarcoma
femur, rib, iliac bone, humerus, tibia
- Chordoma
sacrococcygeal, spheno-occipital, cervical, lumbar, thoracic
-Eosinophilic Granuloma
femur, skull, iliac bone, rib, vertebra
- Enchondroma
phalanges of hands and feet, femur, humerus, metacarpals, rib
-Ewing's sarcoma
femur, iliac bone, fibula, rib, tibia
-Fibrous dysplasia
femur, tibia, rib, skull, humerus
-Giant Cell Tumor
femur, tibia, fibula, humerus, distal radius
- Hemangioma
spine, ribs, craniofacial bones, femur, tibia
- Lymphoma
femur, tibia, humerus, iliac bone, vertebra
- Metastases
vertebrae, ribs, pelvis, femur, humerus
-Non Ossifying Fibroma
tibia, femur, fibula, humerus
-Osteoid osteoma
femur, tibia, spine, tarsal bone, phalanx
-Osteoblastoma
spine, tarsal bone (calc), femur, tibia, humerus
-Osteochondroma
femur, humerus, tibia, fibula, pelvis
-Osteomyelitis
femur, tibia, humerus, fibula, radius
-Osteosarcoma
femur, tibia, humerus, fibula, iliac bone
-Solitary Bone Cyst
proximal humerus, proximal femur, calcaneal bone, iliac bone
http://www.radiologyassistant.nl/en/494e15cbf0d8d
cortical destruction
 Cortical destruction
Cortical destruction-Cortical destruction is a common finding, and not very useful in distinguishing between malignant and benign lesions.
-Complete destruction may be seen in high-grade malignant lesions, but also in locally aggressive benign lesions like EG and osteomyelitis.
-More uniform cortical bone destruction can be found in benign and low-grade malignant lesions. -Endosteal scalloping of the cortical bone can be seen in benign lesions like FD and low-grade chondrosarcoma.The above images show irregular cortical destruction in an osteosarcoma (left) and cortical destruction with aggressive periosteal reaction in Ewing's sarcoma.
 - Ballooning is a special type of cortical destruction. In ballooning the destruction of endosteal cortical bone and the addition of new bone on the outside occur at the same rate, resulting in expansion.
- Ballooning is a special type of cortical destruction. In ballooning the destruction of endosteal cortical bone and the addition of new bone on the outside occur at the same rate, resulting in expansion.-This 'neocortex' can be smooth and uninterrupted, but may also be focally interrupted in more aggressive lesions like GCT.
left: Chondromyxoid fibroma A benign, well-defined, expansile lesion with regular destruction of cortical bone and a peripheral layer of new bone.
right: Giant cell tumor A locally aggressive lesion with cortical destruction, expansion and a thin, interrupted peripheral layer of new bone. Notice the wide zone of transition towards the marrow cavity, which is a sign of aggressive behavior.
 Cortical destruction (3)
Cortical destruction (3)-In the group of malignant small round cell tumors which include Ewing's sarcoma, bone lymphoma and small cell osteosarcoma, the cortex may appear almost normal radiographically, while there is permeative growth throughout the Haversian channels.These tumors may be accompanied by a large soft tissue mass while there is almost no visible bone destruction.The image on the left shows an Ewing's sarcoma with permeative growth through the Haversian channels accompanied by a large soft tissue mass. The radiograph does not shown any signs of cortical destruction.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Aggressive periosteal reaction
 Aggressive periosteal reaction (2)
Aggressive periosteal reaction (2)- left: Osteosarcoma with interrupted periosteal rection and Codman's triangle proximally. There is periosteal bone formation perpendicular to the cortical bone and extensive bony matrix formation by the tumor itself.
-middle: Ewing sarcoma with lamellated and focally interrupted periosteal reaction. (blue arrows)
- right: Infection with a multilayered periosteal reaction. Notice that the periostitis is aggressive, but not as aggressive as in the other two cases.
-Fibrous dysplasia, Enchondroma, NOF and SBC are common bone lesions.They will not present with a periosteal reaction unless there is a fracture. If no fracture is present, these bone tumors can be excluded.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Aggressive periosteal reaction
 Aggressive periosteal reaction
Aggressive periosteal reaction -This type of periostitis is multilayered, lamellated or demonstrates bone formation perpendicular to the cortical bone.
-It may be spiculated and interrupted - sometimes there is a Codman's triangle.
-A Codman's triangle refers to an elevation of the periosteum away from the cortex, forming an angle where the elevated periosteum and bone come together.
-In aggressive periostitis the periosteum does not have time to consolidate.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
benign periosteal reaction

Benign periosteal reaction in an osteoid osteoma
Benign periosteal reaction
- Detecting a benign periosteal reaction may be very helpful, since malignant lesions never cause a benign periosteal reaction.
- A benign type of periosteal reaction is a thick, wavy and uniform callus formation resulting from chronic irritation.
-In the case of benign, slowly growing lesions, the periosteum has time to lay down thick new bone and remodel it into a more normal-appearing cortex.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
periosteal reaction
 Periosteal reaction
Periosteal reaction-A periosteal reaction is a non-specific reaction and will occur whenever the periosteum is irritated by a malignant tumor, benign tumor, infection or trauma.
-There are two patterns of periosteal reaction: a benign and an aggressive type.
-The benign type is seen in benign lesions such as benign tumors and following trauma.
-An aggressive type is seen in malignant tumors, but also in benign lesions with aggressive behavior, such as infections and eosinophilic granuloma.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
age versus types of bone tumors
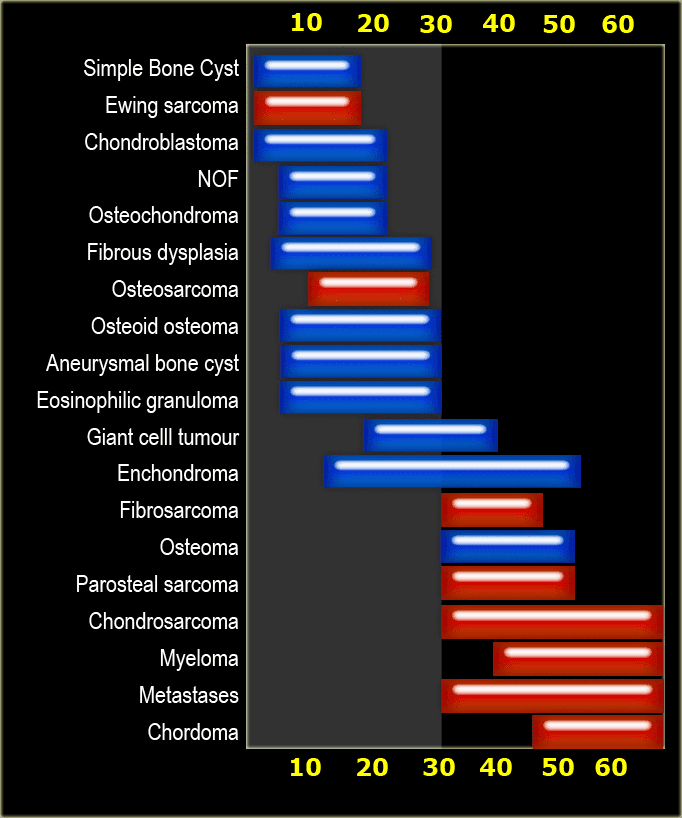 Table: specific tumors by age : Malignant bone tumors in red and benign tumors in blue
Table: specific tumors by age : Malignant bone tumors in red and benign tumors in blueAge:
-Age is the most important clinical clue in differentiating possible bone tumors.There are many ways of splitting age groups, as can be seen in this table.
-Some prefer to divide patients into two age groups: <> 30 years.
-Most primary bone tumors are seen in patients <> 30 years we must always include metastases and myeloma in the differential diagnosis.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
wide zone of transition
 Wide zone of transition
Wide zone of transition -An ill-defined border with a broad zone of transition is a sign of aggressive growth . It is a feature of malignant bone tumors.-
-There are two tumor-like lesions which may mimic a malignancy and have to be included in the differential diagnosis. These are infections and eosinophilic granuloma. Both of these entities may have an aggressive growth pattern.
-Infections and eosinophilic granuloma are exceptional because they are benign lesions which may seem malignant due to their aggressive biologic behavior. These lesions may have ill-defined margins, but cortical destruction and an aggressive type of periosteal reaction may also be seen.
-EG almost always occurs in patients < 30 years and has to be included in the differential diagnosis of any bone lesion in a patient < 30 years.
-Infections have to be included in the differential diagnosis of any bone lesion at any age.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
small zone of transition
Small zone of transition
- A small zone of transition results in a sharp, well-defined border and is a sign of slow growth.
-A sclerotic border especially indicates poor biological activity.
-In patients <> 30years, and particularly over 40 years, despite benign radiographic features, metastasis or plasmacytoma also have to be considered
On the above three bone lesions with a narrow zone of transition. Based on the morphology and the age of the patients, these lesions are benign. Notice that in all three patients, the growth plates have not yet closed.
-In patients > 40 years metastases and multiple myeloma are the most common bone tumors.
-Metastases under the age of 40 are extremely rare, unless a patient is known to have a primary malignancy. Metastases could be included in the differential diagnosis if a younger patient is known to have a malignancy, such as neuroblastoma, rhabdomyosarcoma or retinoblastoma.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
zone of transition
Zone of transition
-In order to classify osteolytic lesions as well-defined or ill-defined, we need to look at the zone of transition between the lesion and the adjacent normal bone.
-The zone of transition is the most reliable indicator in determining whether an osteolytic lesion is benign or malignant .
-The zone of transition only applies to osteolytic lesions since sclerotic lesions usually have a narrow transition zone.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
-In order to classify osteolytic lesions as well-defined or ill-defined, we need to look at the zone of transition between the lesion and the adjacent normal bone.
-The zone of transition is the most reliable indicator in determining whether an osteolytic lesion is benign or malignant .
-The zone of transition only applies to osteolytic lesions since sclerotic lesions usually have a narrow transition zone.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
systemic approach
 In the table on the above the morphology of a bone lesion is combined with the age of the patient.
In the table on the above the morphology of a bone lesion is combined with the age of the patient.Notice the following:
-Infections, a common tumor mimic, are seen in any age group. Infection may be well-defined or ill-defined osteolytic, and even sclerotic.
-EG and infections should be mentioned in the differential diagnosis of almost any bone lesion in patients < 30 years.
- Many sclerotic lesions in patients > 20 years are healed, previously osteolytic lesions which have ossified, such as: NOF, EG, SBC, ABC and chondroblastoma.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
systemic approach

Most bone tumors are osteolytic. The most reliable indicator in determining whether these lesions are benign or malignant is the zone of transition between the lesion and the adjacent normal bone .
Once we have decided whether a bone lesion is sclerotic or osteolytic and whether it has a well-defined or ill-defined margins, the next question should be: how old is the patient? Age is the most important clinical clue. Finally other clues need to be considered, such as a lesion localization within the skeleton and within the bone, any periosteal reaction, cortical destruction, matrix calcifications, etc.
systemic approach
 The most important determinators in the analysis of a potential bone tumor are:
The most important determinators in the analysis of a potential bone tumor are:The morphology of the bone lesion on a plain radiograph
-Well-defined osteolytic
- ill-defined osteolytic
-Sclerotic
-The age of the patient
It is important to realize that the plain radiograph is the most useful examination for differentiating these lesions. CT and MRI are only helpful in selected cases.
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Sunday, August 8, 2010
BI-RADS category 3
 BI-RADS 3. Non-palpable sharply defined lesion with a cluster of punctate calcifications.
BI-RADS 3. Non-palpable sharply defined lesion with a cluster of punctate calcifications.BI-RADS 3Probably Benign Finding - Initial Short-Interval Follow-Up Suggested:
A finding placed in this category should have less than a 2% risk of malignancy.
It is not expected to change over the follow-up interval, but the radiologist would prefer to establish its stability.Lesions appropriately placed in this category include:
-Nonpalpable, circumscribed mass on a baseline mammogram (unless it can be shown to be a cyst, an intramammary lymph node, or another benign finding),
- Focal asymmetry which becomes less dense on spot compression view
-Cluster of punctate calcifications
The initial short-term follow-up is a unilateral mammogram at 6 months, then a bilateral follow-up examination at 12 months and 24 months after the initial examination.
If the findings shows no change in the follow up the final assessment is changed to BI-RADS 2 (benign) and no futher follow up is needed.
http://www.radiologyassistant.nl/en/4349108442109#a43d222d3b66d9
 BI-RADS 2
BI-RADS 2Benign Finding:Like BI-RADS 1, this is a normal assessment, but here, the interpreter chooses to describe a benign finding in the mammography report. Involuting, calcified fibroadenomas, multiple secretory calcifications, fat-containing lesions such as oil cysts, lipomas, galactoceles and mixed-density hamartomas all have characteristically benign appearances, and may be labeled with confidence.
The interpreter may also choose to describe intramammary lymph nodes, vascular calcifications, implants or architectural distortion clearly related to prior surgery, while still concluding that there is no mammographic evidence of malignancy.
http://www.radiologyassistant.nl/en/4349108442109#a43d222d3b66d9
 BI-RADS 1
BI-RADS 1Negative:There is nothing to comment on.
The breasts are symmetric and no masses, architectural distortion or suspicious calcifications are present.
http://www.radiologyassistant.nl/en/4349108442109#a43d222d3b66d9
BI-RADS category 0
 BI-RADS 0 at screening.
BI-RADS 0 at screening.Additional ultrasound after referral was performed allowing final assessment.
Need Additional Imaging Evaluation and/or Prior Mammograms For Comparison
http://www.radiologyassistant.nl/en/4349108442109#a43d222d3b66d9
mammographic breast composition
Mammographic Breast Composition
Mammographic breast composition is described as follows:
1. the breast is almost entirely fat (<25% glandular)
2. scattered fibroglandular densities (25-50%)
3. heterogeneously dense breast tissue (51-75%)
4. extremely dense (> 75% glandular)
http://www.radiologyassistant.nl/en/4349108442109
Mammographic breast composition is described as follows:
1. the breast is almost entirely fat (<25% glandular)
2. scattered fibroglandular densities (25-50%)
3. heterogeneously dense breast tissue (51-75%)
4. extremely dense (> 75% glandular)
http://www.radiologyassistant.nl/en/4349108442109


Subscribe to:
Comments (Atom)


