 MRI T1, precontrast showing solitary myeloma involving the second cervical vertebra,notice the T1 hypointensity.
MRI T1, precontrast showing solitary myeloma involving the second cervical vertebra,notice the T1 hypointensity.D.D.:
Spinal metastases.

 Blue arrow points to "continuous diaphragm sign." The entire diaphragm is visualized from one side to the other because air in the mediastinum outlines the central portion which is usually obscured by the heart and mediastinal soft tissue structures that are in contact with the diaphragm. The red arrow points to the air beneath and posterior to the heart
Blue arrow points to "continuous diaphragm sign." The entire diaphragm is visualized from one side to the other because air in the mediastinum outlines the central portion which is usually obscured by the heart and mediastinal soft tissue structures that are in contact with the diaphragm. The red arrow points to the air beneath and posterior to the heart 19-year-old man with blunt tracheal rupture. Anteroposterior chest radiograph shows large right-sided pneumothorax, pneumomediastinum, subcutaneous emphysema, and chest wall injuries (arrowheads).
19-year-old man with blunt tracheal rupture. Anteroposterior chest radiograph shows large right-sided pneumothorax, pneumomediastinum, subcutaneous emphysema, and chest wall injuries (arrowheads). This chest radiograph shows pneumomediastinum (radiolucency noted around the left heart border) in this patient who had a respiratory and circulatory arrest in the ED after experiencing multiple episodes of vomiting and a rigid abdomen. The patient was taken immediately to the operating room, where a large rupture of the esophagus was repaired.
This chest radiograph shows pneumomediastinum (radiolucency noted around the left heart border) in this patient who had a respiratory and circulatory arrest in the ED after experiencing multiple episodes of vomiting and a rigid abdomen. The patient was taken immediately to the operating room, where a large rupture of the esophagus was repaired. Posteroanterior chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Mediastinal air is noted adjacent to the anteroposterior window and airtrapping extends to the neck, especially on the right side.
Posteroanterior chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Mediastinal air is noted adjacent to the anteroposterior window and airtrapping extends to the neck, especially on the right side. CT scan of chest showing an anterior mediastinal mass (thymoma) in a patient with myasthenia gravis.
CT scan of chest showing an anterior mediastinal mass (thymoma) in a patient with myasthenia gravis. 2-Mediastinal teratoma: Enhanced CT scan of the chest shows large, septated anterior
2-Mediastinal teratoma: Enhanced CT scan of the chest shows large, septated anterior  3-Substernal thyroid. Axial contrast-enhanced CT scan reveals an enlarged thyroid gland extending inferiorly to the level of, and posterior to, the sternum (arrow). There is mass effect on the trachea, which is compressed and displaced toward the right.
3-Substernal thyroid. Axial contrast-enhanced CT scan reveals an enlarged thyroid gland extending inferiorly to the level of, and posterior to, the sternum (arrow). There is mass effect on the trachea, which is compressed and displaced toward the right. 4-Mediastinal lymphoma: Esophageal involvement by mediastinal lymphoma. CT scan in a patient with large cell lymphoma of the mediastinum shows extensive mediastinal adenopathy compressing the esophagus (arrowhead) and superior vena cava (arrow).
4-Mediastinal lymphoma: Esophageal involvement by mediastinal lymphoma. CT scan in a patient with large cell lymphoma of the mediastinum shows extensive mediastinal adenopathy compressing the esophagus (arrowhead) and superior vena cava (arrow).  1) Pulmonary Alveolar Edema. There is extensive, bilateral airspaces disease with fluid in the minor fissure (blue arrow) and bilateral pleural effusions (ref arrows). Although the heart is not enlarged, the cause was still on a cardiogenic basis.
1) Pulmonary Alveolar Edema. There is extensive, bilateral airspaces disease with fluid in the minor fissure (blue arrow) and bilateral pleural effusions (ref arrows). Although the heart is not enlarged, the cause was still on a cardiogenic basis. 2) pneumonia
2) pneumonia 3) aspiration pneumonia:Ninety percent of unilateral diffuse lung opacities are accounted for by just five conditions: pneumonia; aspiration; pulmonary oedema; lymphangitis; and radiation pneumonitis.
3) aspiration pneumonia:Ninety percent of unilateral diffuse lung opacities are accounted for by just five conditions: pneumonia; aspiration; pulmonary oedema; lymphangitis; and radiation pneumonitis. 4)pulmonary hemorrhage:chest radiographs demonstrate extensive bilateral diffuse pulmonary consolidation with sparing of the periphery of the lungs, creating the window frame effect that is suggestive of pulmonary hemorrhage.
4)pulmonary hemorrhage:chest radiographs demonstrate extensive bilateral diffuse pulmonary consolidation with sparing of the periphery of the lungs, creating the window frame effect that is suggestive of pulmonary hemorrhage. Hysterosalpingogram in 40-year-old woman shows medium-sized cesarean section scar defect arising from left lower uterine cavity wall (arrow).
Hysterosalpingogram in 40-year-old woman shows medium-sized cesarean section scar defect arising from left lower uterine cavity wall (arrow). Tubal polyp. Spot radiograph shows a small filling defect (arrow) in the proximal left fallopian tube, a finding that typically represents a tubal polyp.
Tubal polyp. Spot radiograph shows a small filling defect (arrow) in the proximal left fallopian tube, a finding that typically represents a tubal polyp. a
a b
b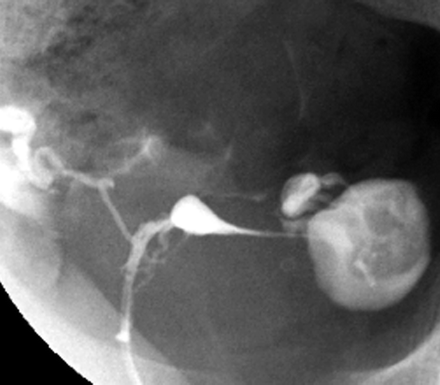 Peritubal adhesions. Spot radiograph demonstrates a round collection of contrast material adjacent to the left fallopian tube, a finding that suggests peritubal adhesions. Note the free contrast material spillage on the right side.
Peritubal adhesions. Spot radiograph demonstrates a round collection of contrast material adjacent to the left fallopian tube, a finding that suggests peritubal adhesions. Note the free contrast material spillage on the right side. a
a
 a
a b
b
 Cornual spasm. (a) On an HSG spot radiograph obtained during the early filling stage of the uterus, the right fallopian tube does not opacify beyond the cornual portion (arrow), whereas the left fallopian tube opacifies to the ampullary portion. Arrowheads indicate amorphous calcifications on the right side of the pelvis. These calcifications were also present on the scout image (not shown). (b) On a spot radiograph obtained after the instillation of additional contrast material, the right fallopian tube opacifies to the ampullary portion. Right-sided SIN and a left-sided hydrosalpinx are also noted. Amorphous calcifications (arrowheads) are again seen on the right side of the pelvis.
Cornual spasm. (a) On an HSG spot radiograph obtained during the early filling stage of the uterus, the right fallopian tube does not opacify beyond the cornual portion (arrow), whereas the left fallopian tube opacifies to the ampullary portion. Arrowheads indicate amorphous calcifications on the right side of the pelvis. These calcifications were also present on the scout image (not shown). (b) On a spot radiograph obtained after the instillation of additional contrast material, the right fallopian tube opacifies to the ampullary portion. Right-sided SIN and a left-sided hydrosalpinx are also noted. Amorphous calcifications (arrowheads) are again seen on the right side of the pelvis.  SIN. Spot radiograph demonstrates SIN as small outpouchings or diverticula from the isthmic portion of the fallopian tubes. SIN can be either unilateral or (as in this case) bilateral.
SIN. Spot radiograph demonstrates SIN as small outpouchings or diverticula from the isthmic portion of the fallopian tubes. SIN can be either unilateral or (as in this case) bilateral. Cesarean section scar. Spot radiograph shows the uterine incision from a cesarean section (arrows) in the typical location (ie, oriented transverse in the lower uterine segment in the region of the isthmus). At HSG, a cesarean section scar can have a linear appearance (as in this case) or can occasionally manifest as a wedge-shaped outpouching or diverticulum.
Cesarean section scar. Spot radiograph shows the uterine incision from a cesarean section (arrows) in the typical location (ie, oriented transverse in the lower uterine segment in the region of the isthmus). At HSG, a cesarean section scar can have a linear appearance (as in this case) or can occasionally manifest as a wedge-shaped outpouching or diverticulum. a
a b
b c
c d
d a
a b
b c
c
 Endometrial polyp. Sagittal sonohysterogram shows a large, well-defined mass in the fundus arising from the anterior aspect of the endometrium. Note the cystic area in the lower portion of the polyp.
Endometrial polyp. Sagittal sonohysterogram shows a large, well-defined mass in the fundus arising from the anterior aspect of the endometrium. Note the cystic area in the lower portion of the polyp. Uterine folds. HSG spot radiograph demonstrates uterine folds (arrows) as linear filling defects that parallel the longitudinal axis of the uterus. Uterine folds are normal findings that are occasionally seen at HSG.
Uterine folds. HSG spot radiograph demonstrates uterine folds (arrows) as linear filling defects that parallel the longitudinal axis of the uterus. Uterine folds are normal findings that are occasionally seen at HSG. Septate and arcuate uterus. Spot radiograph demonstrates a depression of the uterine fundus, a finding that may represent a short septum or an arcuate deformity.
Septate and arcuate uterus. Spot radiograph demonstrates a depression of the uterine fundus, a finding that may represent a short septum or an arcuate deformity. Bicornuate uterus. Spot radiograph shows two markedly splayed uterine horns. The fallopian tubes are not visualized at this imaging stage.
Bicornuate uterus. Spot radiograph shows two markedly splayed uterine horns. The fallopian tubes are not visualized at this imaging stage. Hysterosalpingography (left image): The contrast material passes the tube from a single unicornate uterus (arrow) to the peritoneal cavity.
Hysterosalpingography (left image): The contrast material passes the tube from a single unicornate uterus (arrow) to the peritoneal cavity. Uterus, müllerian duct abnormalities. Surgically proven case of bicornuate uterus. Correct diagnosis may be suggested based on hysterosalpingography findings, which are, most notably, the widened intercornual distance (>4 cm) and the widened intercornual angle (>60°).
Uterus, müllerian duct abnormalities. Surgically proven case of bicornuate uterus. Correct diagnosis may be suggested based on hysterosalpingography findings, which are, most notably, the widened intercornual distance (>4 cm) and the widened intercornual angle (>60°). Uterus, müllerian duct abnormalities. T-shaped uterus. Classic configuration of the uterine cavity in a typical diethylstilbestrol-exposed uterus (American Fertility Society class VII). Uteri are typically hypoplastic. In this patient, no maternal history of diethylstilbestrol exposure was found.
Uterus, müllerian duct abnormalities. T-shaped uterus. Classic configuration of the uterine cavity in a typical diethylstilbestrol-exposed uterus (American Fertility Society class VII). Uteri are typically hypoplastic. In this patient, no maternal history of diethylstilbestrol exposure was found. Hysterosalpingography (left image): Severe dilatation of the tubes following a short intact section (black arrows) is visible. The contrast material cannot get into the peritoneal cavity. Operation is not possible because the intact part of the tube is short.
Hysterosalpingography (left image): Severe dilatation of the tubes following a short intact section (black arrows) is visible. The contrast material cannot get into the peritoneal cavity. Operation is not possible because the intact part of the tube is short. Hysterosalpingography: Normal anatomical structures. The contrast material is injected through a Schultze-device placed into the cervix. The contrast material outlines the uterine cavity and the thin Fallopian tubes opening into the peritoneal cavity.
Hysterosalpingography: Normal anatomical structures. The contrast material is injected through a Schultze-device placed into the cervix. The contrast material outlines the uterine cavity and the thin Fallopian tubes opening into the peritoneal cavity.








{kind=link}
75511-8&usg=__uLfFVRE3__7U0tMAo_b468-jhbc=&h=152&w=200&sz=5&hl=en&start=3&itbs=1&tbnid=jHnWESUzdpIIyM:&tbnh=79&tbnw=104&prev=/images%3Fq%3Dsub%2Bsternal%2Bthyroid,ct%26hl%3Den%26sa%3DG%26gbv%3D2%26tbs%3Disch:1){kind=link}
70542-0&usg=__uTZTDQZoEVoHH4U-pWmSd-gqSmo=&h=194&w=200&sz=6&hl=en&start=13&itbs=1&tbnid=krD-8l90xPz2yM:&tbnh=101&tbnw=104&prev=/images%3Fq%3Dmediastinal%2Blymphoma%26hl%3Den%26sa%3DG%26gbv%3D2%26tbs%3Disch:1){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}