
First, the entire abdomen is examined with a 4- to 5-MHz curved sector scanner. There are a number of other etiologies of abdominal or RLQ pain, ranging from mesenteric adenitis, to obstructive uropathy, to ovarian torsion. Thus, an examination of the entire abdomen is clearly warranted. In women, one must examine the pelvis through a distended bladder with a sector or curved ray scanner. Do not fail to perform an endovaginal examination in female patients if possible pelvic disease exists or if possible abnormalities are identified on the transabdominal scan.
Second, the compression examination is performed with a high-resolution ( ≥ 7.5 MHz) linear array transducer . Patient localization can be added to the study. It has been shown that if the patient points to the location of the pain, this sonographic "self localization" helps reduce examination time and is a valuable addition to the standard graded compression US of the appendix.
ultrasound findings in appendicitis:
1-thickened wall >3mm.
2-diameter >6-7mm.
3-blind ended tubular structure.
4-non compressible.
5-appendicolith.
6-circumfrential color flow.
7-echogenic mesentery.
8-free fluid.
9-abscess.
figure 6
 Ultrasound scanning technique. Linear ray ultrasound probe using compression technique is used to examine the RLQ of the abdomen. The examiner's left hand may be placed poste-rior to the patient's flank to ensure adequate compression.
Ultrasound scanning technique. Linear ray ultrasound probe using compression technique is used to examine the RLQ of the abdomen. The examiner's left hand may be placed poste-rior to the patient's flank to ensure adequate compression.When performing the graded compression, the common femoral artery and vein is identified in order to orient to the RLQ. The patient is then scanned cephalad from this position. The transducer is then used to compress the RLQ, including the terminal ileum and the cecum, to identify any possible appendix. Better compression is obtained if the left hand is placed behind the patient's flank.
The normal appendix may be commonly identified.[23] When visualized, the normal appendix should be a blind-ended, tubular structure with a maximum wall thickness of ¾ 2 mm with an outer diameter of ¾ 6 mm, have no peristalsis, and originate from the base of the cecum. Normal bowel will have peristalsis and thus change lumen size (figure 7). In most instances, the inner-echogenic submucosal ring and the outer hypoechoic ring may also be helpful to identify the normal appendix, although this pattern may be seen with other segments of the bowel.
figure 7
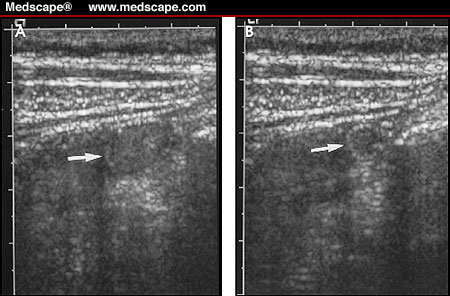 Normal bowel. (A) Ultrasound examination of the RLQ demonstrating 1-cm loop of fluid-filled bowel (arrow). (B) With compression and normal peristalsis, the diameter of this normal loop of bowel decreases to 5 mm (arrow).
Normal bowel. (A) Ultrasound examination of the RLQ demonstrating 1-cm loop of fluid-filled bowel (arrow). (B) With compression and normal peristalsis, the diameter of this normal loop of bowel decreases to 5 mm (arrow).Ultrasound findings of acute appendicitis are listed in Table 2 . These include a blind-ended, noncompressible fluid-filled structure with a wall thickness of ≥ 3 mm and an outer diameter of ≥ 7 mm identified around the appendix (figure 8). There may be a circumferential color-flow identified around the appendix (figure 9). There may also be free fluid noted in the RLQ of the abdomen and the pelvis, and there may be echogenic mesenteric fat (figure 10). If appendiceal perforation has occurred, an ill-defined and/or fluid-filled abscess may be identified. While 6 mm is usually identified as the cutoff between normal and abnormal appendix, in some instances, 5 mm is used as the upper limits of normal, while 7 mm is considered to be positive for acute appendicitis. Thus, in some instances, a measurement between 5 and 7 mm is considered to be equivocal.
figure 8 Acute appendicitis. Ultrasound of the RLQ of the abdomen demonstrating blind-ended tubular structure (open arrows) corresponding to acutely inflamed appendix. Note the distended lumen [L], the echogenic surrounding mesentery [M], and the echogenic structure with acoustic shadow (arrow) at the base of the appendix corresponding to an appendolith.
Acute appendicitis. Ultrasound of the RLQ of the abdomen demonstrating blind-ended tubular structure (open arrows) corresponding to acutely inflamed appendix. Note the distended lumen [L], the echogenic surrounding mesentery [M], and the echogenic structure with acoustic shadow (arrow) at the base of the appendix corresponding to an appendolith.
 Acute appendicitis. Ultrasound of the RLQ of the abdomen demonstrating blind-ended tubular structure (open arrows) corresponding to acutely inflamed appendix. Note the distended lumen [L], the echogenic surrounding mesentery [M], and the echogenic structure with acoustic shadow (arrow) at the base of the appendix corresponding to an appendolith.
Acute appendicitis. Ultrasound of the RLQ of the abdomen demonstrating blind-ended tubular structure (open arrows) corresponding to acutely inflamed appendix. Note the distended lumen [L], the echogenic surrounding mesentery [M], and the echogenic structure with acoustic shadow (arrow) at the base of the appendix corresponding to an appendolith.figure9 Acute appendicitis. Transverse color-flow ultrasound of the RLQ of the abdomen demonstrates increased vascularity (arrow) in a fluid-filled structure corre-sponding to acute appendicitis. External iliac artery [A] is identified.
Acute appendicitis. Transverse color-flow ultrasound of the RLQ of the abdomen demonstrates increased vascularity (arrow) in a fluid-filled structure corre-sponding to acute appendicitis. External iliac artery [A] is identified.
 Acute appendicitis. Transverse color-flow ultrasound of the RLQ of the abdomen demonstrates increased vascularity (arrow) in a fluid-filled structure corre-sponding to acute appendicitis. External iliac artery [A] is identified.
Acute appendicitis. Transverse color-flow ultrasound of the RLQ of the abdomen demonstrates increased vascularity (arrow) in a fluid-filled structure corre-sponding to acute appendicitis. External iliac artery [A] is identified.figure 10 Acute appendicitis. Ultrasound demon-strating a blind-ended tubular structure with fluid-filled lumen [L]. Also note there is a small amount of fluid [M] surrounding the tip of the appendix.
Acute appendicitis. Ultrasound demon-strating a blind-ended tubular structure with fluid-filled lumen [L]. Also note there is a small amount of fluid [M] surrounding the tip of the appendix.
http://www.medscape.com/viewarticle/431119_4
 Acute appendicitis. Ultrasound demon-strating a blind-ended tubular structure with fluid-filled lumen [L]. Also note there is a small amount of fluid [M] surrounding the tip of the appendix.
Acute appendicitis. Ultrasound demon-strating a blind-ended tubular structure with fluid-filled lumen [L]. Also note there is a small amount of fluid [M] surrounding the tip of the appendix.http://www.medscape.com/viewarticle/431119_4



No comments:
Post a Comment