
Click on image to enlarge

Langerhans Histiocytosis
Also known as eosinophilic granuloma(tosis)
Proliferative disorder of the Langerhans cells
Normally found in the skin (and a few other organs) and serve as antigen-presenting cells
Rare diseases, affecting neonates up to adults
2:1 male to female predominance
Prognosis
Mortality and morbidity are associated with the clinical presentation and age of onset of the disease
Worst prognosis for neonates presenting with the disseminated form
Three clinical forms
Acute disseminated Langerhans cell histiocytosis (aka Letterer-Siwe disease)
Occurs most frequently in infants 2 years of age or younger (and occasionally adults)
Presents with multi system organ involvement
Cutaneous lesions resembling seborrheic dermatitis involve the scalp, face, trunk and buttocks as the dominant clinical feature (nearly 80% of patient will have this)
Infiltration of bone marrow and other organs lead to concurrent hepatosplenomegaly, lypmhadenopathy, pulmonary lesions, anemia, thrombocytopenia, recurrent infections (otitis media)
Eventually, there are destructive osteolytic bone lesions
If untreated, this disease is rapidly fatal
With chemotherapy, 5 year survival rate is approximately 50 percent
Univocal Langerhans cell histiocytosis (aka Eosinophilic granuloma or granulomatosis)
Usually only affects the skeletal system of young adults
Typically presents as an osteolytic lesion involving the
Calvaria
Vertebra
Rib
Mandible
Femur
Ilium
Scapula
Bony lesions are usually asymptomatic
In some cases, can cause pain and even pathologic fractures
Pulmonary lesions may be the only presenting symptom and organ involved, especially in adults
Skeletal lesion is usually indolent in nature
Can heal spontaneously or be cured by local excision or irradiation
Pulmonary lesions are typically followed and treated with supportive care
Multifocal Langerhans cell histiocytosis (aka Hand-Schuller-Christian disease)
Triad
Diabetes insipidus
Exophtalmos
Holes in the bone, usually the head (calvarium)
Commonly affects children
Can lead to
Lypmhadenopathy
Hepatomegaly
Splenomegally
Diabetes insipidus is secondary to infiltration of the posterior pituitary stalk by the Langerhans cell
About a third of these patients will also display cutaneous lesions
Some will experience spontaneous regression while others can be treated with chemotherapy
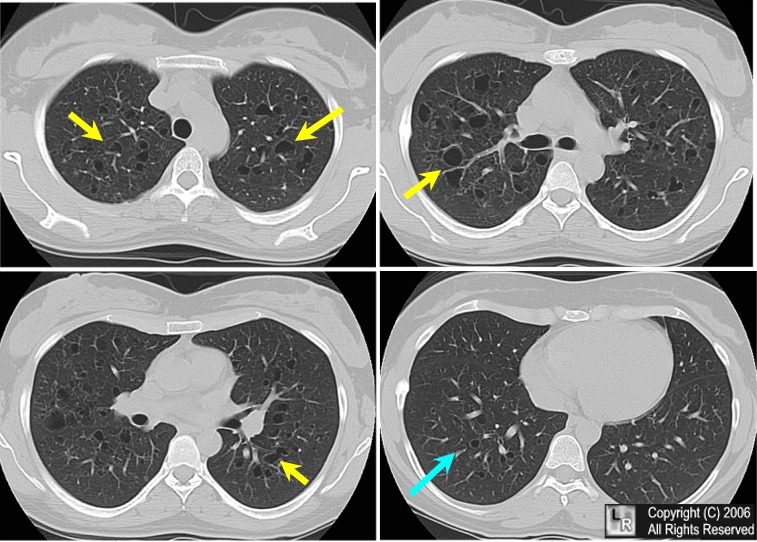
Langerhans histiocytosis (Eosinophilic granuloma of lung). Four selected non-enhanced axial CT scans of the chest show multiple small, irregularly-shaped, cysts of varying sizes with thin walls scattered throughout the lungs (yellow arrows) but predominantly seen in the upper lung fields while sparing the costophrenic angles and lung bases (blue arrow).
Quick Facts
Letterer-Siwe Disease
10% of histiocytosis X
Acute disseminated, fulminant form
Age at onset
Several weeks after birth to 2 years
Pathology
May be confused with leukemia
Symptoms
Hemorrhage, purpura
Severe anemia
Fever
Hepatosplenomegaly and lypmhadenopathy
Bone involvement in 50%
Widespread lytic lesions
Prognosis: 70% mortality rate
Hand-Schuller-Christian
15-40% of Histiocytosis X
Triad of:
Exophthalmos (33%)
Diabetes insipidus (30-50%)
Lytic skull lesions
Pathology
May simulate Ewing's sarcoma
Age at onset
5-10 years
Target organs
Bone
Lytic skull lesions with overlying soft tissue nodules
Large geographic skull lesions
"Floating teeth" with mandibular involvement
Soft tissue
Hepatosplenomegaly is rare
Lypmhadenopathy which may be massive
Lung
Cyst and bleb formation with spontaneous PTX
Ill-defined diffuse nodular disease often leading to fibrosis and honeycombing
Prognosis: spontaneous remissions and exacerbations
Eosinophilic granuloma
60-80% of Histiocytosis X
Usually confined to bone
Age at onset
5-10 years highest frequency
Male predominance 3:2
Location
Calvarium>mandible>spine>ribs>long bones
Most are monostotic (50-75%)
Target organs
Skull (50%)
Diploic space of parietal bone most often
Round or ovoid punched out lesions with beveled edge
Sclerotic margin during healing phase
Beveled edge=hole-within-a-hole
Button sequestrum- bony sequestrum within lytic lesion
Axial skeleton (25%)
"Vertebra plana"-"coin-on-edge"(Calve disease)=collapse of vertebral body, mostly thoracic
Most common cause of vertebra plana in children
Proximal long bones (15%)
Expansile, lytic lesions, mostly diaphyseal
Soft tissue mass
Laminated periosteal reaction
Lung (20%)
Age peak between 20-40 years
Multiple small nodules
Predilection for apices
Prototype for honeycomb lung
Recurrent pneumothoraces (25%)
Rib lesions with fractures common
Nuclear Medicine
Negative bone scans in 35%
Bone lesions usually not Ga-67 avid
Ga-67 may be helpful in detecting non-osseous lesions
Prognosis: excellent



{kind=link}
No comments:
Post a Comment